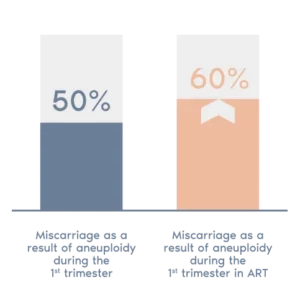
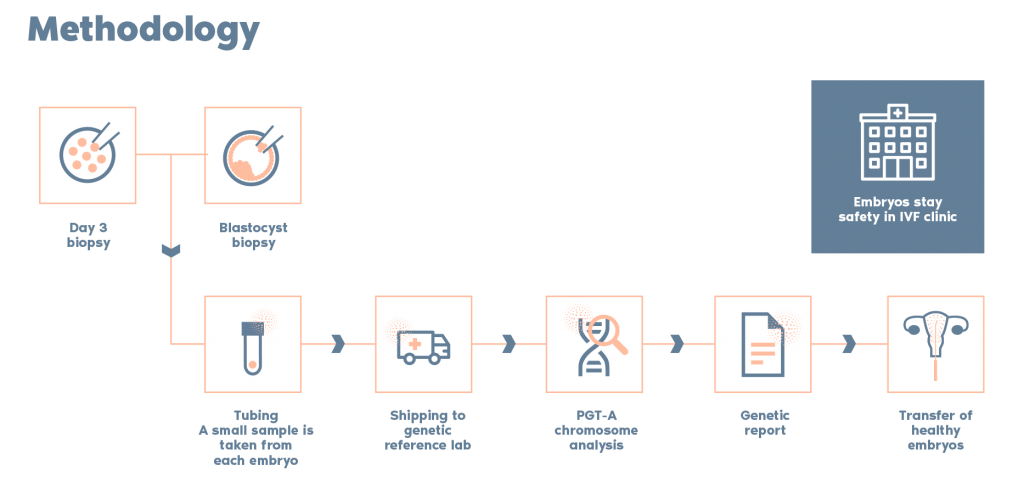
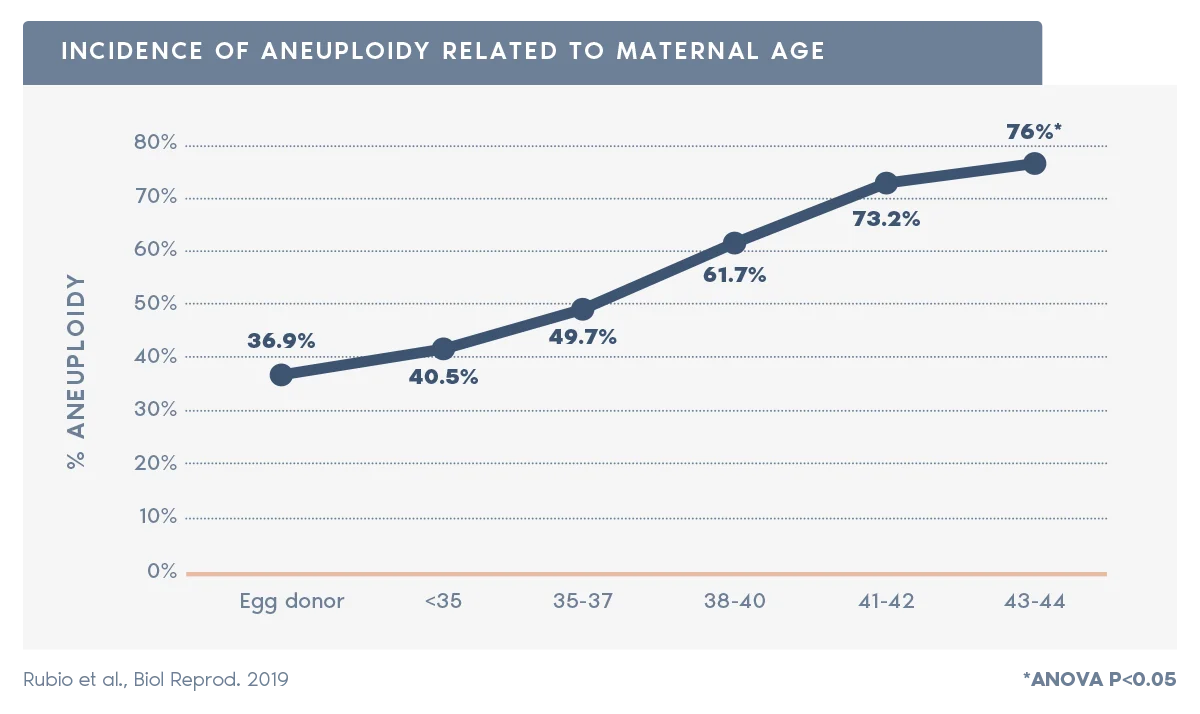
> PGT-A is particularly important for patients over 35, as aneuploidy rate increases with maternal age from approximately 52% at maternal age under 35, to approximately 80%, at age 42.
> PGT-A also can greatly reduce the likelihood of a patient having a multiple-gestation pregnancy by choosing a Single Embryo Transfer (SET).
PGT-A does not test for:
> Birth defects
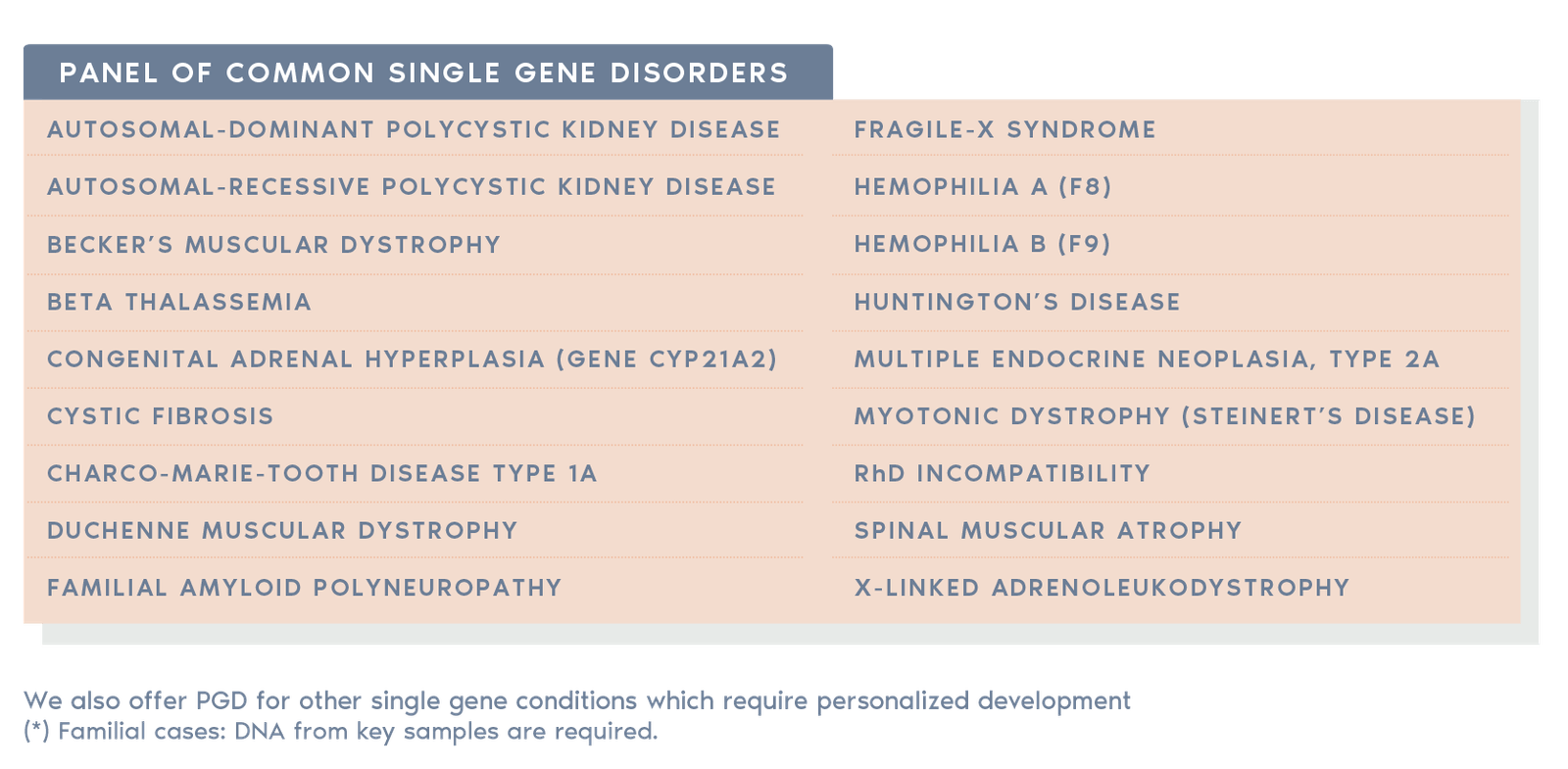
> Inherited single gene disorders, such as cystic fibrosis or Tay-Sachs disease
> Multifactorial conditions, including autism
> Adult-onset conditions such as diabetes or Alzheimer´s disease
> Physical and mental traits, such as intelligence or athleticism
> Microdeletions/microduplications
As with most tests, PGT-A has some limitations:
1. Accuracy is ~98%
> False positive: There is a small chance an embryo could be excluded unnecessarily
> False negative: There is a small chance that an embryo diagnosed as normal could still be chromosomally abnormal
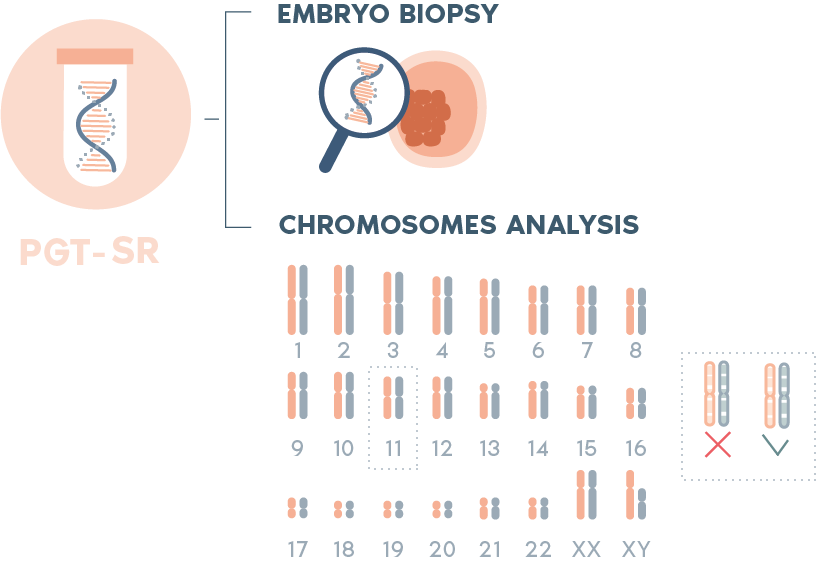
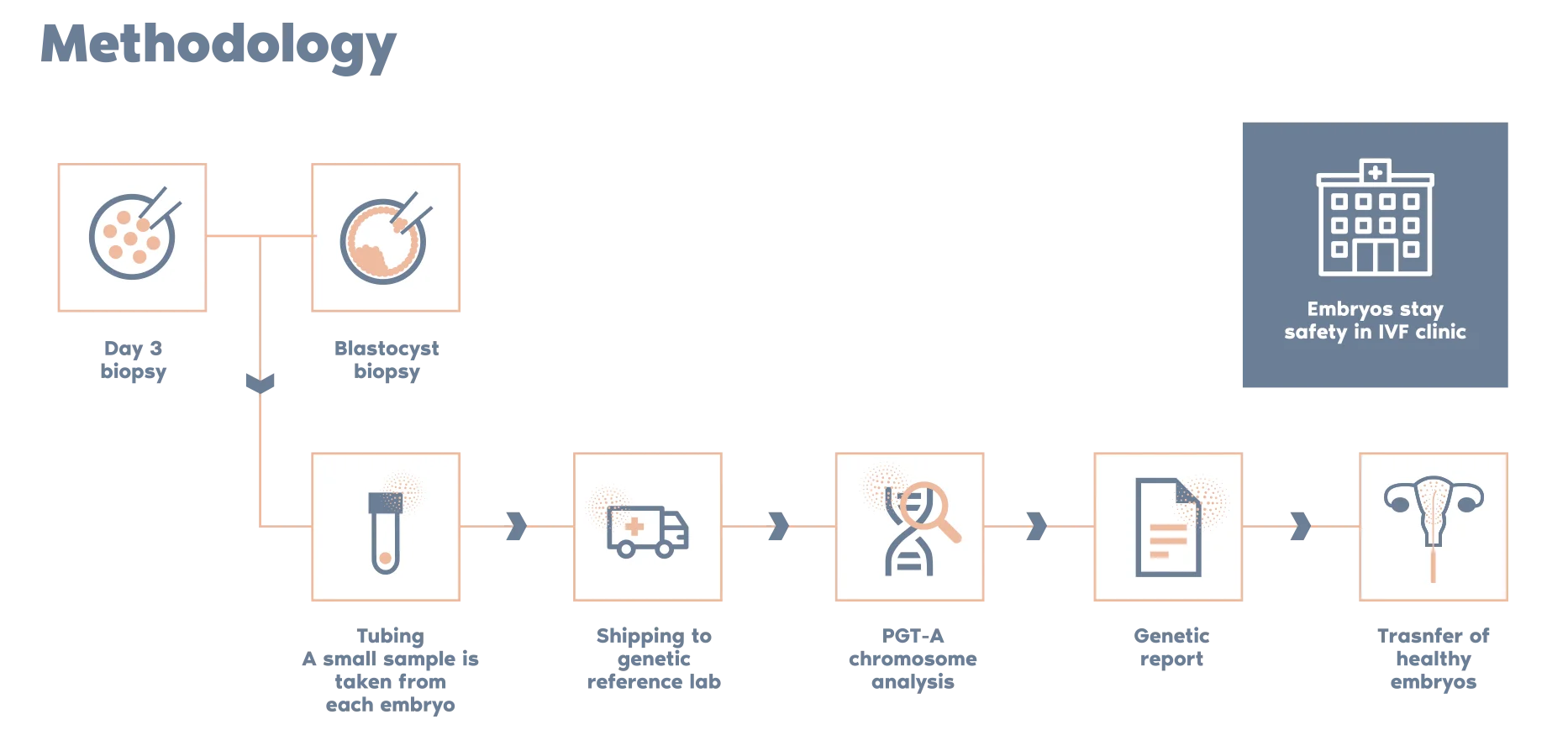
2. PGT-A tests only the samples produced by embryo biopsy, not whole embryos
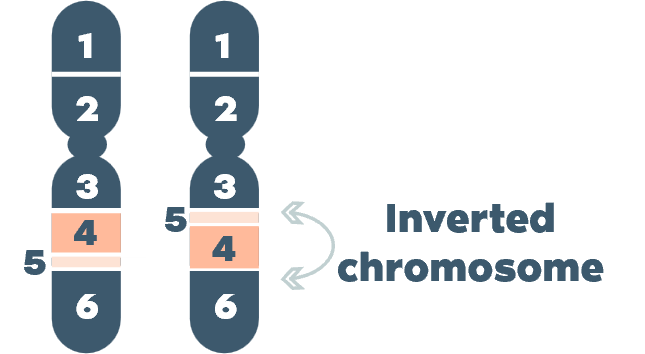
3. PGT-A does not detect structural abnormalities that do not involve gains or losses of genetic material. Additionally, the following cannot be detected:
> Chromosome losses/gains bellow 10Mb,
> Low level of mosaicism (<30%)
> Uniparental disomy (UDP)
> Defects affecting the complete set of chromosomes (haploidy, triploidy)
Follow-up prenatal testing is recommended to confirm the results of PGT-A.
There is a chance of unforeseeable problems with transportation, such as weather and air travel issues, or other circumstances beyond the control of Igenomix that may delay the reporting of results.
In a small percentage of cases, genetic testing cannot be performed due to improper biopsy techniques, loss of biopsied cells, or poor DNA quality.